
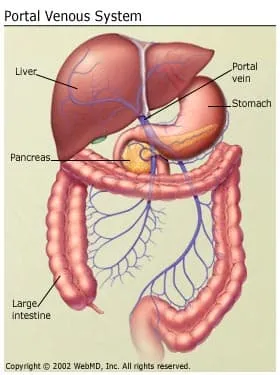
Portal hypertension is an increase in the blood pressure within a system of veins called the portal venous system. Veins coming from the stomach, intestine, spleen, and pancreas merge into the portal vein, which then branches into smaller vessels and travels through the liver. If the vessels in the liver are blocked due to liver damage, blood cannot flow properly through the liver. As a result, high pressure in the portal system develops. This increased pressure in the portal vein may lead to the development of large, swollen veins (varices) within the esophagus, stomach, rectum, or umbilical area (belly button). Varices can rupture and bleed, resulting in potentially life-threatening complications.
What Causes Portal Hypertension?
The most common cause of portal hypertension is cirrhosis of the liver. Cirrhosis is scarring which accompanies the healing of liver injury caused by hepatitis, alcohol, or other less common causes of liver damage. In cirrhosis, the scar tissue blocks the flow of blood through the liver.
Other causes of portal hypertension include blood clots in the portal vein, blockages of the veins that carry the blood from the liver to the heart, a parasitic infection called schistosomiasis, and focal nodular hyperplasia, a disease seen in people infected with HIV, the virus that may lead to AIDS. Sometimes the cause is unknown.
What Are the Symptoms of Portal Hypertension?
The onset of portal hypertension may not always be associated with specific symptoms that identify what is happening in the liver. But if you have liver disease that leads to cirrhosis, the chance of developing portal hypertension is high.
The main symptoms and complications of portal hypertension include:
- Gastrointestinal bleeding marked by black, tarry stools or blood in the stools, or vomiting of blood due to the spontaneous rupture and hemorrhage from varices
- Ascites (an accumulation of fluid in the abdomen)
- Encephalopathy or confusion and forgetfulness caused by poor liver function
- Reduced levels of platelets, blood cells that help form blood clots, or white blood cells, the cells that fight infection
How Is Portal Hypertension Diagnosed?
Usually, doctors make the diagnosis of portal hypertension based on the presence of ascites or of dilated veins or varices as seen during a physical exam of the abdomen or the anus. Various lab tests, X-ray tests, and endoscopic exams may also be used.
How Is Portal Hypertension Treated?
Unfortunately, most causes of portal hypertension cannot be treated. Instead, treatment focuses on preventing or managing the complications, especially the bleeding from the varices. Diet, medications, endoscopic therapy, surgery, and radiology procedures all have a role in treating or preventing the complications. Other treatment depends on the severity of the symptoms and on how well your liver is functioning.
Treatment may include:
- Endoscopic therapy. This is usually the first line of treatment for variceal bleeding and consists of either banding or sclerotherapy. Banding is a procedure in which a gastroenterologist uses rubber bands to block off the blood vessel to stop bleeding. Sclerotherapy is occasionally used when banding cannot be used and is a procedure in which a blood-clotting solution is injected into the bleeding varices to stop bleeding.
- Medications. Nonselective beta-blockers (nadolol or propranolol) may be prescribed alone or in combination with endoscopic therapy to reduce the pressure in varices and further reduce the risk of bleeding. Nonselective beta blockers are also prescribed to prevent a first variceal hemorrhage in a patient with varices that are felt to be at risk for bleeding. Esophageal variceal banding has also been used for that purpose, especially in patients who can't take beta blockers. The drug lactulose can help treat confusion and other mental changes associated with encephalopathy. Diuretics can be prescribed for fluid buildup.
What Lifestyle Changes Should Be Made for Portal Hypertension?
Maintaining good nutritional habits and keeping a healthy lifestyle may help you avoid portal hypertension. Some of the things you can do to improve the function of your liver include the following:
- Do not use alcohol or street drugs.
- Do not take any over-the-counter or prescription drugs or herbal medicines without first consulting your doctor or nurse. (Some medications may make liver disease worse.)
- Follow the dietary guidelines given by your health care provider, including eating a low-sodium (salt) diet. You will probably be required to consume no more than 2 grams of sodium per day. Reduced protein intake may be required if confusion is a symptom. A dietitian can create a meal plan for you.
Other Treatment Options for Portal Hypertension
If endoscopic therapy, drug therapy, and/or dietary changes don't successfully control variceal bleeding or ascites (a buildup of fluid in your belly), you may require one of the following procedures to reduce the pressure in these veins. Decompression procedures include:
- Transjugular intrahepatic portosystemic shunt (TIPS): This procedure involves placing a stent (a tubular device) in the middle of the liver. The stent connects the hepatic vein with the portal vein, which reroutes blood flow in the liver and helps relieve pressure in abnormal veins.
- Distal splenorenal shunt (DSRS): Less common these days, this procedure connects the vein from your spleen to the vein from the left kidney in order to reduce pressure in the varices and control bleeding.
What Tests Might Be Performed Before the TIPS and DSRS Procedures?
Before receiving either of these procedures for portal hypertension, the following tests may be performed to determine the extent and severity of your condition:
- Evaluation of your medical history
- A physical exam
- Blood tests
- Angiogram (an X-ray test that takes pictures of the blood flow within a particular artery)
- Ultrasound
- Endoscopy
Before either the TIPS or DSRS procedure, your doctor may ask you to have other tests, which may include an electrocardiogram (EKG) (a test that records the electrical activity of your heart), chest X-ray, or additional blood tests. If your doctor thinks you will need additional blood products (such as plasma), they will be ordered at this time.
What Happens During the TIPS Procedure?
During the TIPS procedure, a radiologist makes a tunnel through the liver with a needle, connecting the portal vein to one of the hepatic veins (veins connected to the liver). A metal stent is placed in this tunnel to keep it open.
The procedure reroutes blood flow in the liver and reduces pressure in abnormal veins, not only in the stomach and esophagus, but also in the bowel and the liver.
This is not surgery. The radiologist performs the procedure within the vessels under X-ray guidance. The process lasts one to three hours, but you should expect to stay in the hospital overnight after the procedure.
How Successful Is the TIPS Procedure?
The TIPS procedure controls bleeding immediately in more than 90% of patients with portal hypertension. However, in about 20% of patients, the shunt may narrow, causing varices to re-bleed at a later time.
What Complications Are Associated With TIPS?
Shunt narrowing or blockage can occur within the first year after the TIPS procedure. Follow-up ultrasound exams are performed frequently after the TIPS procedure to detect these complications. The signs of a blockage include increased ascites (accumulation of fluid in the abdomen) and re-bleeding. This condition can be treated by a radiologist who re-expands the shunt with a balloon or repeats the procedure to place a new stent.
Encephalopathy, or abnormal functioning of the brain, can occur with severe liver disease. Hepatic encephalopathy can become worse when blood flow to the liver is reduced by TIPS, which may result in toxic substances reaching the brain without being metabolized first by the liver. This condition can be treated with medications, diet, or by making the shunt inaccessible.
What Happens in the DSRS Procedure?
The DSRS is a surgical procedure during which the vein from the spleen (called the splenic vein) is detached from the portal vein and attached to the left kidney (renal) vein. This surgery selectively reduces the pressure in the varices and controls the bleeding associated with portal hypertension. It is usually performed only in patients with good liver function.
A general anesthetic is given before the surgery, which lasts about four hours. You should expect to stay in the hospital from seven to 10 days following surgery.
How Successful Is the DSRS Surgery?
The DSRS procedure provides good long-term control of bleeding in many people with portal hypertension. DSRS controls bleeding in more than 90% of patients, with the highest risk of any re-bleeding occurring in the first month.
What Complications Are Associated With DSRS Surgery?
Ascites, an accumulation of fluid in the abdomen, can occur with DSRS surgery. This can be treated with diuretics and by restricting sodium in the diet.
Follow-Up Care Following TIPS or DSRS Procedures
Follow-up care for TIPS and DSRS can differ depending on where the procedures are performed. Here are basic guidelines:
- Ten days after hospital discharge, meet with your surgeon or hepatologist (liver specialist) to evaluate your progress. Lab work will likely be done at this time.
- Six weeks after the TIPS procedure (and again three months after the procedure), an ultrasound is often done so your doctor can check that the shunt is functioning properly. You may have an angiogram (an X-ray of blood vessels) if the ultrasound indicates that there is a problem. You will also likely have lab work done at these times.
- Six weeks after the DSRS procedure (and again three months after the procedure), the surgeon will evaluate your progress. Lab work may be done at these times.
- Six months after either the TIPS or DSRS procedure, an ultrasound may be done to make sure the shunt is working properly.
- Twelve months after either procedure, another ultrasound of the shunt is often done. Also, you may have an angiogram so that your doctor can check the pressure within the veins across the shunt.
- If the shunt is working well, every six months after the first year of follow-up appointments, you may have an ultrasound, lab work, and visit with your doctor.
- More frequent follow-up visits may be necessary, depending on your condition.
Attend all follow-up appointments as scheduled to ensure that the shunt is functioning properly. Be sure to follow the dietary recommendations that your health care providers give you.
Attend all follow-up appointments as scheduled to ensure that the shunt is functioning properly. Be sure to follow the dietary recommendations that your health care providers give you.
Other Treatments for Portal Hypertension
- Liver transplant. This is done in cases of end-stage liver disease.
- Devascularization. A surgical procedure that removes the bleeding varices; this procedure is done when a TIPS or a surgical shunt is not possible or is unsuccessful in controlling the bleeding.
- Paracentesis. This is a procedure in which the accumulation of fluid in the abdomen (ascites) is directly removed. The results are usually temporary and the procedure will need to be repeated as needed.