
Decline in mental processes is a complication of advanced HIV infection.
- Although the specific symptoms vary from person to person, they may be part of a single disorder known as AIDS dementia complex, or ADC. Other names for ADC are HIV-associated dementia and HIV/AIDS encephalopathy.
- Common symptoms include decline in thinking, or "cognitive," functions such as memory, reasoning, judgment, concentration, and problem solving.
- Other common symptoms are changes in personality and behavior, speech problems, and motor (movement) problems such as clumsiness and poor balance.
- When these symptoms are severe enough to interfere with everyday activities, a diagnosis of dementia may be warranted.
AIDS dementia complex typically occurs as the CD4+ count falls to less than 200 cells/microliter. It may be the first sign of AIDS. With the advent of antiretroviral therapy (ART), the frequency of ADC has declined. ART may not only prevent or delay the onset of AIDS dementia complex in people with HIV infection, it can also improve mental function in people who already have ADC.
Causes of AIDS Dementia
AIDS dementia complex is caused by the HIV virus itself, not by the opportunistic infections that occur commonly in advanced HIV. We do not know exactly how the virus damages brain cells.
HIV may affect the brain through several mechanisms. Viral proteins may damage nerve cells directly or by infecting inflammatory cells in the brain and spinal cord. HIV may then induce these cells to damage and disable nerve cells. HIV causes generalized inflammation, which can cause memory issues, as well as other aging processes, including heart disease.
Symptoms of AIDS Dementia
AIDS dementia complex can affect behavior, memory, thinking, and movement. At first, symptoms are subtle and may be overlooked, but they gradually become troublesome. The symptoms vary widely from person to person.
Symptoms of early dementia include:
- Reduced productivity at work
- Poor concentration
- Mental slowness
- Difficulty learning new things
- Changes in behavior
- Decreased libido
- Forgetfulness
- Confusion
- Word-finding difficulty
- Apathy (indifference)
- Withdrawal from hobbies or social activities
- Depression
Initially subtle disease can progress to more severe symptoms such as:
- Sleep disturbances
- Psychosis -- Severe mental and behavioral disorder, with features such as extreme agitation, loss of contact with reality, inability to respond appropriately to the environment, hallucinations, delusions
- Mania -- Extreme restlessness, hyperactivity, very rapid speech, poor judgment
- Seizures
Without ART, these symptoms gradually worsen. They can lead to a vegetative state, in which the person has minimal awareness of his or her surroundings and is incapable of interacting.
AIDS Dementia Exams and Tests
In a person who's known to have HIV infection, cognitive, behavioral, or motor symptoms suggests that the person might have ADC. It's important to consider, however, other possible causes of these symptoms, such as metabolic disorders, infections, degenerative brain diseases, stroke, tumor, and many others. Your healthcare provider will carry out an evaluation to determine the cause of your symptoms. This will likely include a medical interview, physical and mental status exams, CT or MRI scans, neuropsychological testing, and, possibly, a spinal tap.
Imaging Studies
CT scan and MRI may detect changes in the brain that support the diagnosis of AIDS dementia complex. Brain changes in ADC worsen over time, so these studies may be repeated periodically. Importantly, these scans help rule out other potentially treatable conditions such as infection, stroke, and brain tumor.
A CT scan or an MRI gives a detailed, 3-dimensional picture of the brain. These scans can show brain atrophy (shrinkage) that is consistent with ADC as well as changes in the appearance of different parts of the brain.
Lab Tests
No lab test confirms the diagnosis of AIDS dementia complex. If you have lab tests, they serve to rule out conditions that might cause similar symptoms. You may have blood drawn for multiple tests.
Your healthcare provider may test your cerebrospinal fluid (CSF). This clear fluid is made in normal cavities in the brain called ventricles, which are seen on a CT scan or an MRI. The fluid surrounds the brain and spinal cord. It cushions and protects these structures and may distribute both beneficial and harmful substances. CSF can be tested for various abnormalities that are related to dementia symptoms. A sample of the CSF is obtained with a lumbar puncture, also called a spinal tap. This procedure involves removal of a sample of CSF from the spinal canal in the lower back.
Electroencephalography
For electroencephalography (EEG), a series of electrodes are attached to the scalp. The electrical activity of the brain is read and recorded. In the later stages of ADC, the electrical activity (which appears as waves) is slower than normal. EEG also is used to see whether a person is having seizures.
Neuropsychological Testing
Neuropsychological testing is the most accurate method of pinpointing and documenting your cognitive abilities. This can help give a more accurate picture of the problems and thus can help in treatment planning. It might be repeated later to monitor changes in symptoms.
The testing involves answering questions and performing tasks that have been carefully prepared for this purpose. The test is given by a neurologist, psychologist, or other specially trained professional. It addresses your ability to think mood, anxiety level, and experience of delusions or hallucinations.
Testing assesses cognitive abilities such as:
- Memory
- Attention
- Orientation to time and place
- Use of language
- Abilities to carry out various tasks and follow instructions
Reasoning, abstract thinking, and problem solving are also tested.
Treatment of AIDS Dementia
Just as there is no cure for AIDS, there is no cure for AIDS dementia complex. However, ADC can be controlled in some people by other appropriate treatments; the most important treatment is effective ART.
Home Care for AIDS Dementia
If you have AIDS dementia complex you should remain physically, mentally, and socially active as long as you are able.
- Stay active. Daily physical exercise helps maximize body and mental functions and maintains a healthy weight. This can be as simple as a daily walk.
- Engage in as much mental activity as you can handle. Keeping your mind working may help keep cognitive problems to a minimum. Puzzles, games, reading, and safe hobbies and crafts are good choices.
- Don't stop seeing your friends and relatives. Your social life is not only enjoyable but keeps your mind active and your emotions in balance.
A balanced and nutritious diet that includes plenty of fruits and vegetables helps maintain a healthy weight and prevent malnutrition and constipation. You should not smoke both for health and safety reasons.
Medical Treatment for AIDS Dementia
Combination antiretroviral therapy (ART), which is effective in controlling HIV infection, also protects many HIV-positive people from developing AIDS dementia complex. In cases of advanced HIV in which ADC is present, ART can partially or completely reduce symptoms of ADC.
No specific treatment is available for cognitive decline in AIDS. Specific symptoms such as depression and behavioral disturbances are sometimes relieved by drug therapy.
- Antidepressant drugs may improve symptoms of depression.
- Antipsychotic drugs may help improve severe agitation or aggression, hallucinations, or delusions.
These "psychoactive" drugs are not appropriate for everyone. Your health care provider may consult a specialist in brain disorders (neurologist or psychiatrist) to determine the best treatment.
Next Steps for AIDS Dementia
If you have AIDS dementia complex, you should have regular and frequent visits with your health care provider. These visits allow repeat testing to monitor your condition, review of symptoms, and adjustments to treatment if needed. The visits also permit the health care provider to assess whether your care is appropriate.
Persons with advanced dementia may require inpatient care in a nursing home or similar facility.
Prevention of AIDS Dementia
Combination antiretroviral therapy (ART) can delay or prevent the development of AIDS dementia complex in people with HIV infection, especially if it is given early in the course of the disease. There is no other known way of preventing ADC.
Outlook for AIDS Dementia
In people who already have advanced HIV and ADC, combination ART will likely result in some improvement in symptoms. If there is no response to ART, the outlook may be poor. For some, the dementia worsens over a period of months until the person is no longer able to care for himself. He or she becomes bedridden, unable to communicate, and dependent on others for care.
Support Groups and Counseling
AIDS dementia complex can be one of the most difficult of all HIV/AIDS complications for you and those who care for you. The condition affects every aspect of your life, including family relationships, work, financial status, social life, and physical and mental health. You may feel overwhelmed, depressed, frustrated, angry, or resentful.
While understandable, these feelings do not help the situation and usually make it worse. This is why support groups were invented. Support groups are groups of people who have lived through the same difficult experiences and want to help themselves and others by sharing coping strategies.
Support groups meet in person, on the telephone, or on the Internet. The following organizations may help you find a support group that is right for you. You can also ask your health care provider or behavior therapist, or go on the Internet. If you do not have access to the Internet, go to the public library.
For More Information
Centers for Disease Control and Prevention, National Prevention Information Network
(800) HIV-0440 (800-448-0440)
(888) 480-3739 TTY
1-301-519-0459 International
Email: [email protected]
Web Site: npin.cdc.gov
Family Caregiver Alliance/National Center on Caregiving
(800) 445-8106
Email: [email protected]
Web Site: www.caregiver.org
National Alliance for Caregiving
(301) 718-8444
Email: [email protected]
Web Site: www.caregiving.org
Multimedia
Media file 1: CT scan of the brain of a patient with AIDS dementia complex (ADC) shows diffuse atrophy (loss of tissue) and ventricular enlargement and attenuation (dark areas) around the ventricles in the white matter.

Media type: CT
Media file 2: T2-weighted MRI shows ventricular enlargement and large areas of hyperintense signal in the subcortical white matter of both frontal lobes.

Media type: MRI
Media file 3: Photomicrograph from a patient with AIDS dementia complex (ADC) shows perivascular and parenchymal infiltrates of lymphocytes and macrophages. These often form microglial nodules. Contributed by Dr. Beth Levy, Saint Louis University School of Medicine, St. Louis.
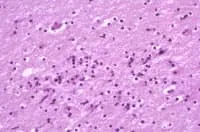
Media type: Photo
Media file 4: Photomicrograph from patient with AIDS dementia complex (ADC) illustrates the intense astrogliosis (scarring) that is characteristic of HIV encephalitis. Contributed by Dr. Beth Levy, Saint Louis University School of Medicine, St. Louis.
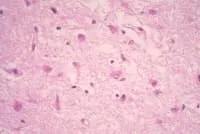
Media type: Photo
Media file 5: Multinucleated giant cells, as shown here, are a hallmark of HIV encephalitis and harbor the virus. Contributed by Dr. Beth Levy, Saint Louis University Health Sciences Center, St. Louis.
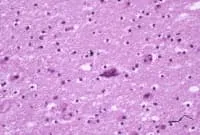
Media type: Photo
Synonyms and Keywords
acquired immunodeficiency syndrome, ADC, AIDS, AIDS dementia complex, AIDS encephalopathy, AIDS-related dementia, HIV-associated cognitive/motor complex, HIV-associated dementia complex, HIV dementia, HIV encephalitis, HIV encephalopathy, HIV infection, HIV-1 infection, dementia due to HIV infection, dementia, combination antiretroviral therapy, ART, HIV, human immunodeficiency virus
