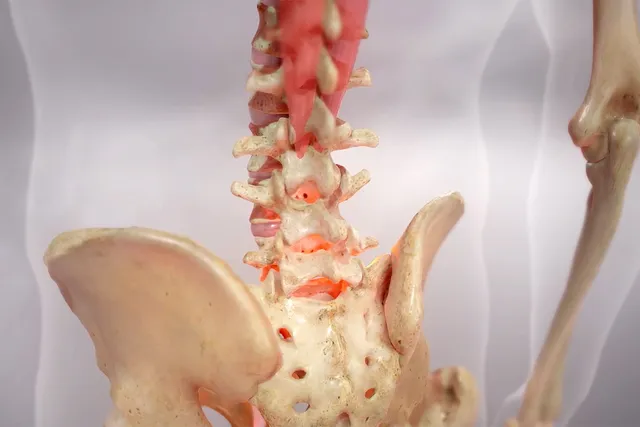
If you have non-radiographic axial spondyloarthritis (nr-axSpA), you may wonder if you’ll get ankylosing spondylitis (AS). That’s when your doctor can see certain bone changes on an X-ray -- they don’t show up when you have nr-axSpA.
Studies show anywhere from 8% to 40% of people with nr-axSpA may get AS within 2 to 10 years. But experts disagree on what this information means for how the disease progresses. Some think nr-axSpA is an early form of AS. Others view them as either distinct conditions or diseases on the same spectrum.
“There’s been lots of arguments in the community,” says Philip Robinson, MBChB, PhD, a rheumatologist and associate professor at The University of Queensland Australia.
Research is ongoing into the link between these conditions. Here’s what we know so far.
Does Non-radiographic-axSpA Become Ankylosing Spondylitis?
Eric Ruderman, MD, PhD, professor of medicine at Northwestern University’s Feinberg School of Medicine, doesn’t think nr-axSpA is simply “pre-ankylosing spondylitis.” He describes them as “two parallel pathways.”
The line between the two blurs in the early stages of the disease. One way to think about it is that everyone with AS goes through the non-radiographic phase. But only a certain number get AS. Early on, doctors can’t tell the difference between the two. And it can take years to find out.
“The nature of inflammation is you don’t go from being well, and then overnight, develop erosions in bone,” Robinson says. “That takes a long time.”
The good news is doctors are starting to catch non-radiographic changes earlier. In the future, scientists may know how to spot specific factors that lead to AS. But we’re not there yet.
What Genes Are Linked to Ankylosing Spondylitis?
The vast majority of people with AS test positive for the HLA-B27 gene. HLA-testing is often used to support a diagnosis of AS, but it can’t tell you if you’ll definitely get the disease later on.
“If you take a group of (people) with non-radiographic disease, those who test positive for HLA-B27 are more likely to develop AS,” Phillips says. “But the predictive value of that in a single person is quite low.”
Ali Ajam, MBBS, a rheumatologist with The Ohio State University Wexner Medical Center, says HLA-B27 has “negative predictive value.” That means there’s a good chance you don’t have AS if you test negative. But a positive result can’t forecast disease transition.
“More than 95% of people who have the gene will not go on to develop AS,” Ajam says. “But on the flip side, if someone has ankylosing spondylitis, more than 95% will have a positive test.”
There’s “some connection” with HLA-B27, Ruderman says. But experts agree there’s no one factor that leads to AS. It’s likely that many genes mix with your environment in a way that triggers an immune reaction. Scientists are still trying to figure out what sets off these biological dominoes.
Who Is More Likely to Get Ankylosing Spondylitis?
No one knows for sure who’ll go from non-radiographic disease to AS. But there are certain risk factors that raise your odds. Other than HLA-B27, some big ones are:
- A family history of AS
- Being male
- Inflammatory markers in your blood
- Active inflammation on your MRI
If you’ve got all these, Ajam says it’s reasonable to have a “low threshold” for thinking there’s a chance nr-axSpA may go into AS.
Can Treatment Prevent Ankylosing Spondylitis?
Biologic drugs, such as TNF-inhibitors, are used to treat inflammation in nr-axSpA and AS. Early data show these meds may “possibly prevent radiographic changes in the spine,” Robinson says. But scientists haven’t studied nr-axSpA long enough to know for sure. Right now, doctors don’t suggest biologics for everyone.
“If you have very minor symptoms, we don’t know enough about progression to know if it’s worth it,” Robinson says.
If you have mild nr-axSpA, it’s likely you’ll start off with physical therapy and nonsteroidal anti-inflammatory drugs (NSAIDs). You may go on to more aggressive treatment if your pain and inflammation are serious. That could include TNF-inhibitors or other disease-modifying drugs (DMARDs).
To pair you with the right treatment, your doctor may run blood tests and give you an MRI. They’ll want to check for signs of active disease, “so you know that you’re in fact treating inflammation that’s going to respond to the biologic,” Ruderman says.
Treat Your Symptoms, Not Your Diagnosis
You may hear people say nr-axSpA is a less severe version of AS. But you can have pain, stiffness, and trouble doing daily things without any radiographic changes. You deserve treatment for the symptoms you have now, not what your X-rays show.
“People who are going to progress or people who aren’t going to progress may be just as affected by disease,” Ruderman says.
In addition to hip and back pain, you may have problems with the small joints in your hands and feet, Ajam says, along with non-joint related issues such as uveitis (inflammation of the eye), inflammatory bowel diseases, or skin diseases like psoriasis.
Ruderman says women are often underdiagnosed. And many of them make up more of the nr-axSpA crowd, which doesn’t show up on X-rays.
“[Some doctors think] if they have normal X-rays, then they must not have bad disease and there’s nothing we should do,” Ruderman says. “But that’s not true because these people can be really impacted.”
Show Sources
Photo Credit: comotion_design / Getty Images
SOURCES:
Philip Robinson, MBChB, PhD, associate professor, The University of Queensland, Australia.
Eric M. Ruderman, MD, professor of medicine (rheumatology), associate chief, clinical affairs for the division of rheumatology, Northwestern University Feinberg School of Medicine.
Ali Ajam, MBBS, The Ohio State University Wexner Medical Center.
Rheumatology and Therapy: “Non-Radiographic Axial Spondyloarthritis (nr-axSpA): Advances in Classification, Imaging and Therapy.
Expert Review of Clinical Immunology: “Radiographic progression in non-radiographic axial spondyloarthritis.”
American College of Rheumatology: “Predicting Progression of Non-Radiographic Axial Spondyloarthritis.”
PLOS One: “Spinal radiographic progression in axial spondyloarthritis and the impact of classification as nonradiographic versus radiographic disease: Data from the Swiss Clinical Quality Management cohort.”
RMD Open: “Non-radiographic axial spondyloarthritis and ankylosing spondylitis: what are the similarities and differences?”
Annals of the Rheumatic Diseases: “Axial spondyloarthritis: a new disease entity, not necessarily early ankylosing spondylitis.”
UpToDate: “Patient education: Axial spondyloarthritis, including ankylosing spondylitis (Beyond the Basics)”
Spondylitis Association of America: “How Disease Severity, Ethnicity, and HLA-B27 Prevalence Intersect,” “Overview of Ankylosing Spondylitis.”
Lab Tests Online: “Ankylosing Spondylitis.”