
What causes osteoarthritis?
Primary osteoarthritis is caused by the breakdown of cartilage, a rubbery material that eases the friction in your joints. It can happen in any joint but usually affects your fingers, thumbs, spine, hips, knees, or big toes.
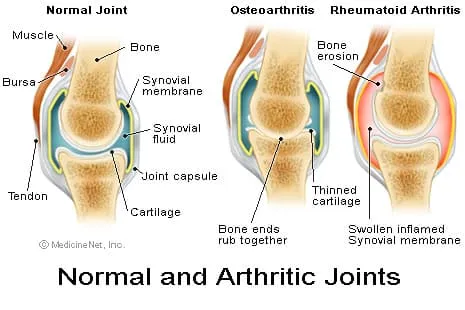
Osteoarthritis is more common in older people. Using your joints over and over damages the cartilage, leading to pain and swelling. Water builds up in the cartilage, and its proteins break down. It may start to flake or get tiny tears. In severe cases, you can lose all the cartilage between the bones of a joint so that they rub together, making it harder and more painful to use the joint.
Cartilage damage can also trigger bone growths (spurs) around your joints.
Osteoarthritis sometimes happens in multiple members of one family, hinting that a gene change has been handed down from parents to children. Rarely, these cases are caused by problems in collagen, a tough protein found in your connective tissue.
Secondary Osteoarthritis Causes and Risk Factors
Secondary osteoarthritis happens when your cartilage is damaged by another disease or medical condition. Things that can cause it or make it more likely include:
- Obesity , which puts more stress on your joints, especially your knees.
- Injury or surgery to the joint. Even if a joint seems to heal the way it should, it’s at higher risk for osteoarthritis later on.
- Unusual joints at birth (congenital abnormalities). These are more likely to wear down, especially in the hip.
- Body mechanics. Things that change the way your body works, such as an unusual way of walking or joints that have a wider range of motion than usual (called hypermobility), can put more stress on them.
- Your job or hobby. Using a joint to make the same motion over and over again -- like squatting or lifting -- may be linked to osteoarthritis.
- Gout. Crystal deposits in the cartilage can cause damage and osteoarthritis. Uric acid crystals cause arthritis in gout, while calcium pyrophosphate crystals cause arthritis in pseudogout.
- Rheumatoid arthritis and other inflammatory conditions of the joints, which lead to joint damage and cartilage breakdown.
- Diabetes and other hormone disorders, which can cause inflammation that leads to osteoarthritis.
- Menopause. Levels of estrogen, which protects your bones and cartilage, fall after menopause.
