
What Is a Salpingectomy?
Salpingectomy (sal-pin-JEK-tuh-me) is the surgical removal of one or both fallopian tubes. After this procedure, getting pregnant is usually more difficult. There are several reasons to get a salpingectomy, such as preventing ovarian cancer, ectopic pregnancy, tubal blockage, or infection.
There are several types of salpingectomy. You may have one or both fallopian tubes removed. Your doctor may recommend removing the entire fallopian tube or only part of it. There are also different surgical approaches: minimally invasive using very small incisions (cuts), or traditional, with a large incision. Your doctor will recommend the best method depending on your situation.
Your fallopian tubes are located on either side of your uterus, at the top, and extend down to your ovaries. The fallopian tubes play an important role in conception. Women or people assigned female at birth (AFAB) ovulate during their menstrual cycle. Ovulation is when your ovary releases an egg for fertilization. The egg is then guided by tiny, finger-like structures through your fallopian tubes towards your uterus. As the egg travels through your fallopian tubes, it can be fertilized by sperm.
Salpingectomy vs. tubal ligation
Tubal ligation is commonly called "getting your tubes tied." “Tubal” refers to the fallopian tubes and “ligation” means to tie. Tubal ligation is any procedure that blocks or interrupts the fallopian tubes. It is done as a permanent form of birth control. During a tubal ligation, your surgeon will either cut the fallopian tubes and tie them with a special thread, cauterize (burn) the edges to seal them with scar tissue, or place clips or bands on the tubes to block them.
Salpingectomy — removing part or all of a fallopian tube — can be considered a type of tubal ligation. If you are having this surgery to prevent pregnancy, you must have a bilateral (both sides) salpingectomy and remove both fallopian tubes. Salpingectomy is done for more reasons than preventing a pregnancy.
Both tubal ligation and salpingectomy can help reduce your risk of ovarian cancer.
How common is female sterilization in the United States?
Each year, about 600,000 surgical sterilizations are performed in the United States. Surgical sterilization, also called permanent contraception (birth control), is the most used method of contraception among people 15-49 years old who are assigned female at birth.
Salpingectomy Types
Types of salpingectomy procedures include:
Partial salpingectomy
A partial salpingectomy is the surgical removal of part of a fallopian tube.
Complete salpingectomy
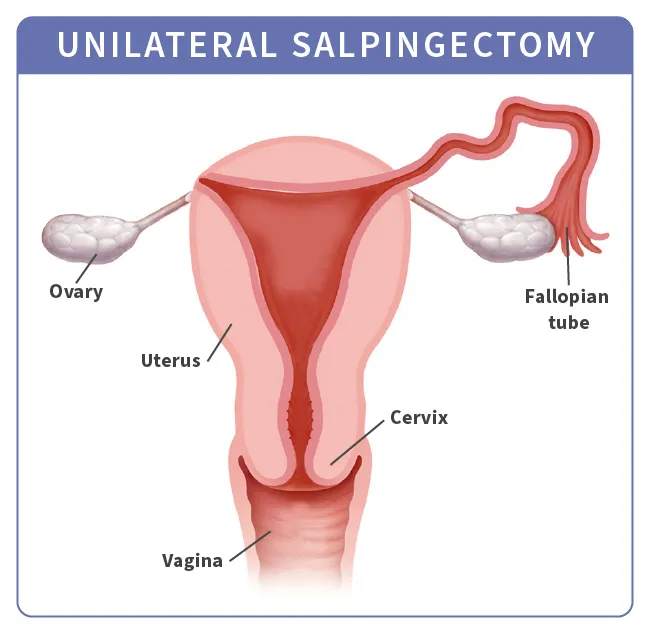
A complete (or total) salpingectomy is a surgical procedure to completely remove one or both fallopian tubes. Removal of one fallopian tube is called a unilateral salpingectomy and removal of both is called a bilateral salpingectomy.
Salpingo-oophorectomy
Oophorectomy is the surgical removal of one or both ovaries. Salpingo-oophorectomy surgery involves removing the fallopian tube and the ovary. It can be unilateral (removal of one fallopian tube and one ovary, usually on the same side) or bilateral (removal of both fallopian tubes and one or both ovaries).
It may be necessary, depending on your condition, to have a hysterectomy with salpingectomy, which means your uterus and cervix will be removed, along with your fallopian tubes. If your ovaries are also removed, this is called a total hysterectomy with bilateral salpingo-oophorectomy.
Salpingectomy with ovarian preservation
Removing only the fallopian tubes and leaving the ovaries is a surgery known as salpingectomy with ovarian preservation. When your ovaries are left in place, you are able to keep estrogen and other hormone levels steady. If you have not yet started menopause, this can prevent early menopause caused by ovary removal.
Opportunistic salpingectomy
Salpingectomy can be done at the same time as another planned abdominal surgery. This is called opportunistic salpingectomy and it simply means taking advantage of the opportunity to remove both fallopian tubes while you are having another abdominal surgery, such as a gallbladder removal or a hernia repair. Even if you don't have a known risk factor for getting ovarian cancer, this surgery can help prevent cancer of the ovary, fallopian tube and peritoneum (the membrane that surrounds the abdominal organs).
Who Might Get a Salpingectomy?
Studies show that 70% of the most common and deadly ovarian cancers begin in the fallopian tubes. Removing the fallopian tubes can help prevent ovarian cancer even while leaving the ovaries intact. Removing your fallopian tubes is recommended only if you are at a higher risk for ovarian cancer or are already planning to have another abdominal or gynecologic surgery.
Many people with the BRCA1 or BRCA2 gene mutations, which cause an increased risk of ovarian and breast cancer, get a salpingectomy.
About 13% of people with breasts get breast cancer. But people with BRCA gene mutations have a 45% to 72% risk of breast cancer. The risk of ovarian cancer is also higher.
Generally, 1.2% of people with uteruses get ovarian cancer. But people with BRCA gene mutations have an 11% to 44% risk of ovarian cancer. Removing the fallopian tubes can reduce the risk of both these cancers.
You may have a higher risk of ovarian cancer if you’ve had breast cancer or if your family has a history of breast, ovarian, pancreatic, or colon cancer. Genetic testing might be recommended. Other gene mutations, such as those associated with Lynch syndrome, have a higher than 1% to 2% lifetime risk of ovarian cancer.
You may also choose to have a salpingectomy if you want to permanently prevent pregnancy. You will need a partial or complete bilateral salpingectomy to prevent pregnancy from occurring naturally. You may still be able to get pregnant by in vitro fertilization (IVF) if you still have a uterus.
Otherwise, people with the following conditions may need a salpingectomy:
- Blocked or damaged fallopian tube
- Ectopic pregnancy
- Endometriosis in the fallopian tubes
- Cancer of the fallopian tubes, uterus, or ovaries
- Antibiotic-resistant fallopian tube infection
Salpingectomy for ectopic pregnancy
An ectopic pregnancy happens when a fertilized egg implants outside of your uterus. The egg is supposed to travel down your fallopian tubes and embed itself into the wall of your uterus, where it can develop. In an ectopic pregnancy, the egg implants before it reaches your uterus. Most ectopic pregnancies happen inside a fallopian tube.
An ectopic pregnancy can quickly become life-threatening. The uterus is the only organ that can stretch to support a growing fetus. If your fallopian tube breaks, it can cause severe bleeding, infection, and sometimes death. This is a medical emergency that must be treated right away.
Health care professionals treat ectopic pregnancies with medications or surgery. The injected medication will stop a fetus from growing and end the pregnancy. A fetus cannot survive outside the uterus and this medication can prevent your fallopian tube from rupturing. If your fallopian tube has already ruptured or is at risk of breaking, surgery is your only option. You'll be placed under general anesthesia and your surgeon will either remove your entire fallopian tube or just the implanted egg.
Salpingectomy and Ovarian Cancer Prevention
Research has shown that many cases of ovarian cancer actually begin in the fallopian tubes. This research also shows that the most aggressive types of ovarian cancer have origins in the fallopian tubes. Some people with uteruses who are at high risk of ovarian cancer elect to have their ovaries, fallopian tubes, or both removed as a preventative measure.
Studies show that a salpingectomy can reduce the risk of ovarian cancer by 42% to 78%. Additionally, getting a salpingectomy with a hysterectomy reduces the risk of ovarian cancer by 50%.
How to Prepare for a Salpingectomy Procedure
Your doctor will review the procedure with you and go over instructions for before and after the surgery. These instructions may vary depending on the type of salpingectomy you're having, your age, and your medical history. If you have an ectopic pregnancy, your salpingectomy is considered an emergency, life-saving procedure.
You will need to let your health care providers know about any medications you take, including prescriptions, over-the-counter drugs, and supplements. These include any medicated patches or creams. You may be asked questions about your health such as how much alcohol you drink, whether you smoke, or if you have sleep apnea. It’s important to answer honestly because these can affect how you respond to anesthesia or surgery.
Before surgery, you will have presurgical testing, which may include blood tests, a chest X-ray, and an electrocardiogram (EKG) to check your heart rhythm. You will be instructed to stop taking aspirin and other nonsteroidal anti-inflammatory drugs (NSAIDs) as well as other supplements, such as fish oil, that can cause bleeding. Don’t stop taking blood thinners without your doctor’s guidance.
You will also be given clear instructions about what to eat, how to shower or bathe, and when to begin fasting (avoiding food) before your surgery. These guidelines are for your safety during surgery.
Salpingectomy Procedure
There are two types of surgical methods used for salpingectomy:
Laparoscopic salpingectomy: A minimally invasive surgery performed using a thin instrument called a laparoscope, which has a light and camera at one end. Your surgeon will insert the laparoscope into your abdomen through a tiny cut called an incision and will inflate your abdomen with a special gas in order to see your uterus and fallopian tubes in detail. Using surgical tools inserted through other small incisions, your surgeon will then remove your fallopian tubes. After removing any excess blood and fluid, your surgeon will close the incisions with stitches or medical glue.
Laparoscopic salpingectomy can be done as a same-day procedure. This means you will not need to be admitted to a hospital and can return home the day of surgery. It’s important to plan ahead and have a ride home after a salpingectomy, since the surgery typically requires general anesthesia.
Open abdominal salpingectomy: A more traditional surgical approach using one large incision across your abdomen (called a laparotomy). Your surgeon will remove your fallopian tubes through this incision. Once your fallopian tubes are removed, your surgeon will stitch or staple the incision closed.
A laparoscopic approach is less invasive, with a shorter recovery time and lower risk of complications. But sometimes an open approach is necessary.
Salpingectomy vs. Oophorectomy
Oophorectomy is the surgical removal of the ovaries. Removing the fallopian tubes but leaving the ovaries may be beneficial. This can delay premature menopause or hormonal changes that follow ovary removal.
Studies have shown that the combination of salpingectomy and an oophorectomy results in the lowest cases of ovarian cancer. However, salpingectomy followed by an oophorectomy later resulted in the best quality of life.
Salpingectomy Recovery
With laparoscopy, the procedure lasts about 1.5 hours. You may go home the same day as the procedure. Most people can go back to work after a few days. After 2 weeks, you can return to all of your normal activities. It is important to follow your surgeon’s instructions after your salpingectomy. Find out from your doctor when it is safe to start having sex again.
It will take longer for you to recover if you had an open abdominal salpingectomy or additional procedures, including a cesarean section (C-section), or went through childbirth. Your recovery may last 4-6 weeks, and your incision site may be sore or painful, making it a challenge to resume your normal activities before you are fully healed.
Some people are concerned about weight gain or weight loss after fallopian tube removal. Salpingectomy does not cause any changes in weight, appetite or appearance. After laparoscopic surgery, your abdomen might be swollen for several days. You may take acetaminophen to relieve pain. Gas in your abdomen might cause discomfort in your neck, shoulders and chest for 24-72 hours after surgery. A warm shower, heating pad, or walking can help.
While you are recovering, seek medical attention if you have any of the following symptoms:
- Painful urination
- Burning when urinating
- Fever
- Chills
- Redness at the incision site
- Swelling at the incision site
- Fluid leaking from the incision
- Excessive bleeding
- Pain that is not helped by medication
- Swelling, redness, or pain in your legs
Salpingectomy Complications
Salpingectomy comes with the risks of any surgery, which include the following:
- Infection
- Damage to the surrounding area
- Blood clots
- Uncontrolled bleeding
- Unexpected reaction to anesthesia
- Hernia
- Scar tissue
Doctors aren't completely sure how the removal of just the fallopian tubes affects hormone production. Studies show that when the tubes are removed for sterilization, hormone production levels of the ovaries don't seem to be affected much. However, if the tubes are removed due to ectopic pregnancy, removal may disrupt the hormone production.
As it is not fully clear how hormone levels can be affected after a salpingectomy, there is a chance of going into premature menopause. But it is lower than that after ovary removal.
Long-term side effects of bilateral salpingectomy
Bilateral salpingectomy, or removal of both fallopian tubes, is considered a permanent form of birth control. If you have a uterus, you can still get pregnant using in-vitro fertilization (IVF). The fallopian tubes aren't responsible for your periods, so if you had periods before your salpingectomy, you'll continue to have them after your surgery.
Most studies of the long-term effects of salpingectomy show that removal of the fallopian tubes is unlikely to have a substantial negative impact on ovarian reserve (the number and quality of eggs for reproduction).
Salpingectomy Considerations
You should discuss with your doctor the risks and benefits of having a salpingectomy. Your medical history, including any previous surgeries, your weight, or certain health conditions may affect your risk factors for the surgery or the method your surgeon may recommend. Because salpingectomy is not reversible, you should carefully consider your decision to have the surgery.
It’s best to avoid making this choice during times of stress (such as during a divorce or after a miscarriage). You should never be pressured into having this surgery by a partner or others. Research shows that women younger than age 30 are more likely than older women to regret having the procedure.
Pregnancy After Salpingectomy
Your fallopian tubes are not responsible for your periods, so you'll continue to have periods after a salpingectomy. If you have a unilateral salpingectomy (removal of just one fallopian tube), you can still get pregnant. You must continue to use contraception to avoid pregnancy if you still have one working fallopian tube.
After having both fallopian tubes removed, you will not be able to get pregnant naturally. However, pregnancy after bilateral salpingectomy is still possible with medical help. After having your fallopian tubes removed, you can get pregnant using in-vitro fertilization (IVF). This process involves collecting eggs from your ovaries, fertilizing them in a lab to create embryos, and then implanting those embryos into your uterus.
The success rate of IVF depends on your age and other health factors. However, one study has shown that there is little difference in IVF success rates between people who have had salpingectomies and those who have not.
Takeaways
Salpingectomy is the surgical removal of one or both fallopian tubes. Studies have shown that removing the fallopian tubes can help prevent ovarian cancer. Salpingectomy is also used to prevent pregnancy and to treat ectopic pregnancy, tubal blockages, endometriosis in the fallopian tubes, and infections.
Salpingectomy FAQs
Why would you have a salpingectomy?
There are several reasons to get a salpingectomy, which is the surgical removal of one or both fallopian tubes. Salpingectomy has been shown to help prevent ovarian cancer, especially in women or people assigned female at birth with a high risk factor, such as the BRCA1 or BRCA2 gene mutation. Salpingectomy is also used as a permanent form of birth control (sterilization) when both fallopian tubes are removed, and as a treatment for ectopic pregnancy, tubal blockage, endometriosis, or infection.
Is a salpingectomy a major surgery?
A salpingectomy can be done as a minimally invasive surgery through small incisions (cuts). This approach is called a laparoscopic salpingectomy. Sometimes it is necessary to perform the surgery through a large incision, a method called open abdominal salpingectomy. Your recovery time for a laparoscopic surgery will be about 2 weeks. An open abdominal salpingectomy takes about 4-6 weeks for recovery. Because both methods require general anesthesia, they may be considered a major surgery. But with a laparoscopic approach, you can usually go home the same day.
What happens to your body when your fallopian tubes are removed?
If you have both fallopian tubes removed (bilateral salpingectomy), you will no longer be able to get pregnant without the help of in-vitro fertilization (IVF). You will still get your period and your ovaries should still function as before. If you had a salpingectomy because of an ectopic pregnancy, your hormone production may be disrupted for a short period of time. After a unilateral salpingectomy (the removal of one fallopian tube) for an ectopic pregnancy, it’s good to talk to your doctor about timing for another pregnancy. Though you may be able to get pregnant again soon after treatment, it’s often best to wait about 3 months. This gives your fallopian tube time to heal and reduces the risk of another ectopic pregnancy.
